
All information is based on current medical research (2018-2026). Written specifically for patient education by Dr. Antonio Gargiulo. This article does not replace a consultation with your gynecologist or healthcare provider.
What is Adenomyosis?
Your uterus (womb) has two main layers: an inner lining called the endometrium, which sheds every month during your period, and a thick muscular outer wall called the myometrium. In adenomyosis, cells that belong only in the inner lining mistakenly grow deep inside the muscle wall of the uterus.
Every month, when your hormones trigger your period, those misplaced cells also bleed and swell — but they have nowhere to go. This causes inflammation, pain, and over time the uterus can grow larger than normal.
Adenomyosis is benign – it is not cancer and does not spread to other organs. It is not rare: studies estimate it affects between 20% and 35% of women, though the true number is hard to pin down because many women have no symptoms at all. Most diagnoses happen between the ages of 32 and 50, but doctors are now finding it in younger women too, thanks to better imaging tools.
Could I Have It? Recognizing the Symptoms
About one in three women with adenomyosis has no symptoms and may only discover the condition during a routine exam or a fertility workup. When symptoms do occur, they can range from mild to life-disrupting.
Heavy menstrual bleeding is the most common complaint. Periods may be so heavy that they cause anemia – a shortage of iron in the blood – leaving you exhausted, dizzy, or short of breath. Research comparing women with adenomyosis to women with endometriosis found that heavy bleeding occurred in 64% of adenomyosis patients, compared to only 19% of those with endometriosis alone. It is the hallmark feature of this disease.
Painful periods (dysmenorrhea) are also very common. For many women, the cramping is far worse than a typical period. The misplaced tissue causes the uterine muscle to contract abnormally and with greater force.
Chronic pelvic pain – a dull, aching, or pressure-like discomfort in the lower abdomen – may persist throughout the month, not just during menstruation.
Painful intercourse (dyspareunia) is reported by many women and can strain intimate relationships.
A feeling of heaviness or bloating in the pelvis can occur when the uterus becomes enlarged – sometimes described as a constant feeling of fullness or pressure in the lower belly.
Fertility problems are also associated with adenomyosis. The disease can interfere with implantation and early pregnancy and has been linked to higher rates of miscarriage and pregnancy complications.
One of the most important things to know: the severity of symptoms does not always match the severity of the disease. Some women with extensive adenomyosis feel very little pain, while others with a mild form suffer greatly. This is one reason the condition is so often misdiagnosed or dismissed for years.
What Causes Adenomyosis?
Scientists do not yet fully understand what causes adenomyosis. Several theories exist, and more than one process may be involved.
Theory 1 – The Invasion Theory (most widely accepted)
The inner lining of the uterus breaks through the boundary between the lining and the muscle wall and begins to grow where it does not belong. This boundary, called the junctional zone, acts like a fence between the two layers. When this fence is damaged – by childbirth, surgery, or repeated microscopic trauma from menstruation – endometrial cells can escape into the muscle. Once there, they trigger inflammation, scarring, and ongoing tissue injury.
Theory 2 – Stem Cell or Embryonic Origin
Adenomyosis may develop from special immature cells (stem cells) present in the uterine muscle since before birth. Under certain hormonal conditions, these cells can transform into tissue that behaves like the uterine lining.
Theory 3 – Invasion from Outside
Some researchers believe adenomyosis can also develop when endometriosis lesions from outside the uterus migrate inward – growing into the uterine wall from the outside.
The role of hormones
All three theories share one common thread: estrogen fuels the disease. Adenomyosis lesions grow in the presence of estrogen and tend to shrink after menopause. Many women also appear to have a reduced response to progesterone, the hormone that normally counteracts estrogen’s effects, allowing the misplaced tissue to keep growing.
Known risk factors include:
– Having had one or more pregnancies
– A history of uterine surgery (cesarean section, D&C, fibroid removal)
– Increasing age (most cases diagnosed between 35 and 50)
– Possible exposure to environmental chemicals (endocrine disruptors) that interfere with hormones
Why a Laparoscopy Cannot Diagnose Adenomyosis
Many women with pelvic pain or heavy bleeding undergo a laparoscopy – a minimally invasive surgery in which a thin camera is inserted through a small incision in the belly button to look inside the pelvis. Laparoscopy is the gold standard for diagnosing endometriosis, because its lesions are visible on the surfaces of pelvic organs. Adenomyosis is fundamentally different: it lives inside the muscle wall of the uterus, entirely out of sight.
From the outside, a uterus with adenomyosis may look completely normal. It does not create visible spots or implants that a surgeon can see. Multiple independent lines of evidence confirm this.
The uterus looks normal from the outside – even to experienced surgeons.
A large 2018 prospective study enrolled patients undergoing laparoscopic hysterectomy and asked expert surgeons to predict whether adenomyosis would be found on final pathology based on how the uterus looked during surgery. The preoperative clinical diagnosis was correct only 51.7% of the time – no better than a coin flip. Not one intraoperative characteristic – shape, color, consistency, or size – significantly predicted adenomyosis. Retrospective video review by three additional blinded expert surgeons found the same result. The conclusion: laparoscopic diagnosis of adenomyosis is inaccurate and unreliable.
Laparoscopy is simply not a diagnostic tool for this disease.
A 2019 review concluded directly that laparoscopy “is not traditionally considered a diagnostic tool for adenomyosis” and can play only a complementary role in ruling out other conditions. The leading international diagnostic framework for adenomyosis – a comprehensive 2020 review in Human Reproduction Update – does not include laparoscopy among the diagnostic tools for this condition at all.
The disease lives in a layer that surgery cannot see.
Adenomyosis involves structural changes in the junctional zone – the inner boundary between the endometrium and the myometrium – that are visible by transvaginal ultrasound and MRI but invisible to any instrument looking at the outside of the uterus. Even under the microscope, confirming adenomyosis requires tissue taken from inside the muscle wall – which means a hysterectomy specimen or a deep myometrial biopsy, not a surface inspection.
What this means for you:
If you have had a laparoscopy that came back “normal” or found only endometriosis, that result says nothing about whether you also have adenomyosis. A normal-looking uterus on the outside does not rule out adenomyosis inside. The right test is a high-quality transvaginal ultrasound or MRI performed by a specialist experienced in recognizing the internal features of this disease.
In conclusion, the following must be stated plainly: if a surgeon’s laparoscopic report describes a diagnosis of adenomyosis – and the findings do not describe deep endometriosis visibly invading the uterine wall from the outside – that report is implicitly wrong. No laparoscopy can diagnose adenomyosis. A surgeon who writes otherwise is, however unintentionally, providing a patient with misleading information. The disease is invisible from the outside. It always has been. The only tools that can find it are imaging from within – transvaginal ultrasound and MRI – or microscopic examination of tissue taken from inside the uterine muscle itself.
How Is Adenomyosis Properly Diagnosed?
Step 1: Medical History and Symptoms
Your doctor will ask detailed questions about your periods, pain levels, reproductive history, and any prior uterine procedures. This clinical picture is the first and most important clue.
Step 2: Transvaginal Ultrasound (TVUS)
This is usually the first test used. A small, smooth probe placed gently inside the vagina produces detailed sound-wave images of the uterus. It is safe, widely available, affordable, and radiation-free. Doctors look for:
– An enlarged or asymmetrically thickened uterus
– Small fluid-filled cysts within the muscle
– Bright or dark streaks within the muscle wall
– An irregular or blurred border between the lining and the muscle
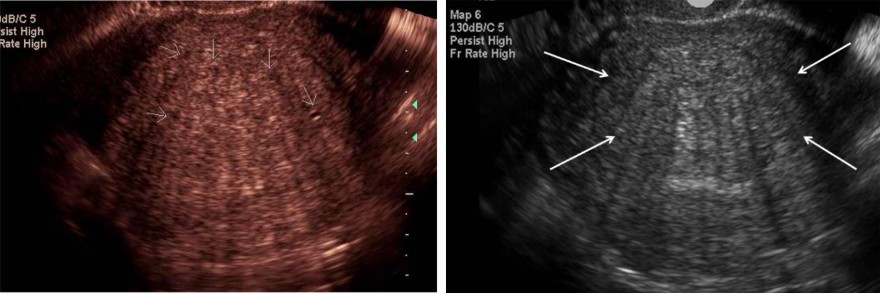
Research shows that transvaginal ultrasound performs comparably to MRI for diagnosing adenomyosis when performed by an experienced sonographer.
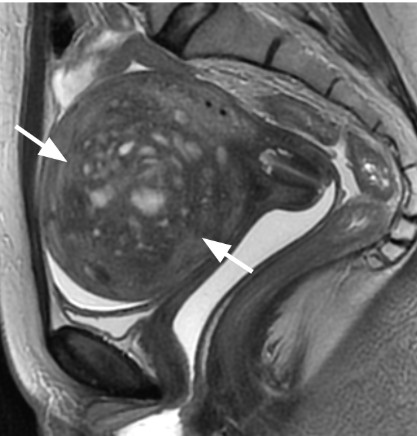
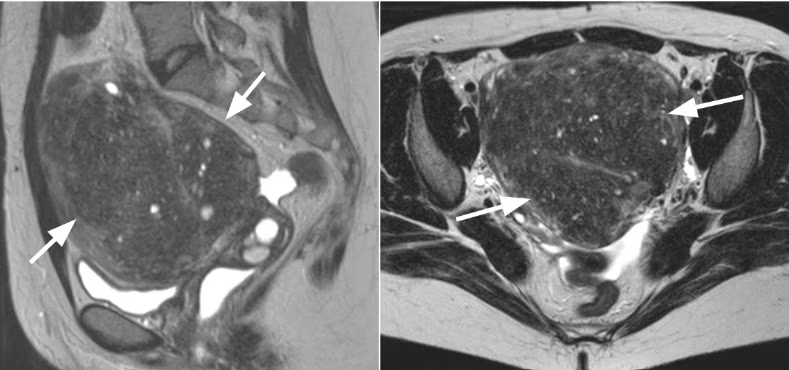
Step 3: Magnetic Resonance Imaging (MRI)
MRI produces highly detailed images using magnetic fields – no radiation. It is particularly useful when ultrasound results are unclear, when fibroids are also present, or when surgery is being planned. It is more expensive and less available than ultrasound but offers excellent detail about the extent and pattern of the disease. Please remember that MRI for endometriosis and adenomyosis is extremely protocol-dependent: only your chosen surgeon should be allowed to prescribe your MRI because they understand how to prepare the patient and who the radiologist should be who reads it. A poorly planned and poorly read MRI can have drastic consequences on your care.
Step 4: Confirming the Diagnosis
In most cases, a clear imaging picture combined with typical symptoms is sufficient to make the diagnosis. Surgery is no longer required simply to confirm the diagnosis.
A definitive microscopic confirmation still requires tissue – from a uterine biopsy or, if other treatments have failed, a hysterectomy.
A Note on Getting Diagnosed
Many women wait years before receiving a correct diagnosis, often because symptoms are attributed to “normal” painful periods, the condition is confused with fibroids or endometriosis, or imaging was not performed or was interpreted by someone inexperienced with adenomyosis. If you have heavy, painful periods that affect your daily life, ask your doctor specifically about adenomyosis and request a transvaginal ultrasound performed in the luteal phase of the menstrual cycle (that is, after ovulation) by a specialist experienced in uterine conditions.
Continue reading: “Adenomyosis and Endometriosis: Two Diseases, One Patient” – understanding how these two conditions overlap, why they are often missed together, and what it means for your quality of life and your care.
Sources We Used
So You Can Read Them, Question Them, and Decide for Yourself
We believe that informed patients are empowered patients. In an age where artificial intelligence and open-access science place original research within reach of anyone, you have every right to go to the source, read it yourself, and form your own conclusions. Patient education on this website is taken seriously: we do not simplify at the cost of truth, and we do not ask you to take our word for it.
Every statement in this article carries two layers of accountability. It has been filtered through the critical eye of Dr. Antonio Gargiulo, drawing on four decades of clinical and surgical experience in reproductive medicine and advanced gynecologic surgery. And it is independently traceable to a peer-reviewed scientific publication, listed below with its full reference and digital identifier (DOI), so you can retrieve and read the original source at any time.
We see healthcare as a shared responsibility between doctors and patients. Shared responsibility requires shared access to information. These references are not a formality. They are here for you.
Kho K, Chen J, Halvorson L. Diagnosis, Evaluation, and Treatment of Adenomyosis. JAMA. 2021. DOI: 10.1001/jama.2020.26436
Bourdon M, Santulli P, Marcellin L, et al. Adenomyosis: an update regarding its diagnosis and clinical features. Journal of Gynecology Obstetrics and Human Reproduction. 2021. DOI: 10.1016/j.jogoh.2021.102228
Schrager S, Yogendran L, Marquez CM, Sadowski E. Adenomyosis: Diagnosis and Management. American Family Physician. 2022.
Gallone A, Santalucia M, Giani M, et al. Adenomyosis and Endometriosis: a differential diagnosis by clinical symptoms. Journal of Endometriosis and Uterine Disorders. 2026. DOI: 10.1016/j.jeud.2026.100153
Chapron C, Vannuccini S, Santulli P, et al. Diagnosing adenomyosis: an integrated clinical and imaging approach. Human Reproduction Update. 2020. DOI: 10.1093/humupd/dmz049
Halvorson L. New Perspectives on Adenomyosis. Seminars in Reproductive Medicine. 2020. DOI: 10.1055/s-0040-1721376
Zhai J, Vannuccini S, Petraglia F, Giudice L. Adenomyosis: Mechanisms and Pathogenesis. Seminars in Reproductive Medicine. 2020. DOI: 10.1055/s-0040-1716687
Guo S-W. Cracking the Enigma of Adenomyosis: An Update on Its Pathogenesis and Pathophysiology. Reproduction. 2022. DOI: 10.1530/REP-22-0224
Stephens VR, Rumph JT, Ameli S, et al. The Potential Relationship Between Environmental Endocrine Disruptor Exposure and the Development of Endometriosis and Adenomyosis. Frontiers in Physiology. 2022. DOI: 10.3389/fphys.2021.807685
Dason ES, Chan C, Sobel M. Diagnosis and treatment of adenomyosis. Canadian Medical Association Journal. 2021. DOI: 10.1503/cmaj.201607
Liu L, Li W, Leonardi M, et al. Diagnostic Accuracy of Transvaginal Ultrasound and Magnetic Resonance Imaging for Adenomyosis. Journal of Ultrasound in Medicine. 2021. DOI: 10.1002/jum.15635
Alcazar JL, Vara J, Usandizaga C, et al. Transvaginal ultrasound versus magnetic resonance imaging for diagnosing adenomyosis: A systematic review and head-to-head meta-analysis. International Journal of Gynaecology and Obstetrics. 2022. DOI: 10.1002/ijgo.14609
Ecker A, Chamsy D, Austin RM, et al. Use of Uterine Characteristics to Improve Fertility-Sparing Diagnosis of Adenomyosis. Journal of Gynecologic Surgery. 2018. DOI: 10.1089/gyn.2017.0112
Pontis A, Nappi L, Sorrentino F, Angioni S. Differential diagnosis of adenomyosis: the role of hysteroscopy and laparoscopy. Clinical and Experimental Obstetrics and Gynecology. 2019. DOI: 10.12891/CEOG4814.2019
Harmsen MJ, Trommelen LM, de Leeuw R, et al. Uterine junctional zone and adenomyosis: comparison of MRI, transvaginal ultrasound and histology. Ultrasound in Obstetrics and Gynecology. 2022. DOI: 10.1002/uog.26117
McCaughey T, Newman M, Constable L, et al. Standardizing the histopathological diagnosis of adenomyosis: an international Delphi consensus. Histopathology. 2025. DOI: 10.1111/his.15480